The TTKG calculator counts the transtubular potassium gradient for you. It is a useful parameter if you want to determine whether or not the distortions in the potassium serum level are due to renal causes. You'll also find a small table of TTKG interpretations, which can give you a useful hint in giving the correct diagnosis.
We try our best to make our Omni Calculators as precise and reliable as possible. However, this tool can never replace a professional doctor's assessment. If any health condition bothers you, consult a physician.
Kidney problem diagnosis - and overview
When diagnosing electrolyte disorders, particularly potassium, the kidneys are the first port of call. Doctors need to assess how they deal with electrolytes to determine if they are the cause. Generally, we use three methods to determine how much of a substance is lost via the kidneys, and whether that amount is appropriate or not. Those are:
- Fractional excretion;
- 24-hour urine test - very often used to assess proteinuria; and
- Transtubular gradient for potassium, like here in this TTKG calculator.
In most cases, like sodium or urea, we would use fractional excretion. Sometimes, like when assessing proteinuria (protein content in the urine), we would choose the 24-hour urine test. Transtubular gradient is used only in case of potassium.
What is transtubular potassium gradient, when, and why do we use it?
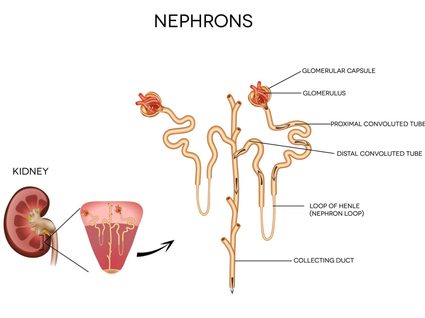
The reason that potassium is an exceptional case is because it is mainly secreted in the distal convoluted tubule, part of a nephron (the functional unit of a kidney). The glomerulus filters a lot of potassium first, but almost all of it gets absorbed right away in the proximal convoluted tubule, any potassium in urine is usually due to the distal convoluted tubule.
Since the fractional excretion is a ratio:
fractional excreation = filtered substance / excreted substance,
we cannot rely on it in this case, as filtered potassium has a little to do with excreted potassium.
This is not the only reason we cannot rely of fractional excretion, however. To accurately count the amount of potassium secreted by the nephrons, we need to make sure there is enough water reabsorbed in the nephron's lumen (which indirectly indicates if the level of antidiuretic hormone - ADH, or vasopressin - is within anormal range). That's why the TTKG formula contains urine and serum osmolality, to measure if vasopressin is working correctly.
Measuring a patient's potassium level with a 24 hours urine sample would be a good choice if it wasn't for... 24 hours. Clinicians usually prefer to have the laboratory test results as fast as possible. Not to mention, for verifying if your treatment is right, you would have to wait another 24 hours.
Summing up all of the above, we need a formula that takes into account not only potassium levels but also normalizes it for the water reabsorption ratio. Transtubular potassium gradient meets both those criteria.
Use of TTKG is limited to states where there are abnormal potassium levels in the serum. So we use it in:
- Hyperkalemia (high K+ level) - to check if the kidneys are excreting potassium effectively; and
- Hypokalemia (low K+ level) - to check if the kidneys are not where the potassium is being lost.
Experts emphasize the use of using TTKG measurements to distinguish between . For further information, scroll down to TTKG interpretation section below.
TTKG formula
The TTKG formula uses four parameters, two measured in urine and two measured in serum.
TTKG = (K+ urine/K+ serum) / (Urine osmolality/Serum osmolality)
where:
- TTKG - transtubular potassium gradient,
- K+ - the amount of potassium ions present.
However, there are some limitations of using this formula:
- The urine osmolality must be at least 300 mOsm/kg H₂O - this is an indirect measure of checking if the level of the hormone vasopressin is ok, which is necessary for the potassium measurements to be accurate
- Urine sodium concentration must be at least 25 mmol/L (or 25 mEq/L) - potassium secretion in the distal collecting tubule depends on the sodium concentration in the urine. If this condition is met, you know that there's enough sodium for the potassium to be adequately secreted in this part of the nephron.
How to use the TTKG calculator?
Using our TTKG calculator is very simple and intuitive. You only need to follow those steps:
- Before using the calculator, make sure the urine sodium concentration is at least equal to 25 mmol/L (or 25 mEq/L). This is required if this formula is to be properly used.
- Input the data from the laboratory test into the calculator.
- Remember, the parameters should be taken from one urine sample and one blood sample. Mixing between samples will only distort your result.
- Thats it! Your result is ready with a quick comment just below the calculator. Remember that the TTKG parameter only gives you information when read together with other parameters, such as the serum potassium concentration. Move on to the section below to learn more.
TTKG interpretation
TTKG result, like every other laboratory tests, cannot be interpreted on their own. You need to take into consideration the patient's potassium serum level, the patient's state, their diet and other renal parameters. The table shows a summary of the possible results with short comments - things to think about and the direction of further diagnosis.
Potassium level (mmol/L) | TTKG | Comment |
|---|---|---|
<3.5 | <3 | normal |
>3 | renal potassium wasting – e.g., hypoaldosteronism, pseudohypoaldosteronism | |
3.5-5 | <8 | TTKG too low¹ |
8-9 | normal if the patient has a normal diet | |
>9 | TTKG too high¹ | |
>5.0 | >7 | normal, but optimally >10 |
<7 | type IV renal tubular acidosis |
¹ In cases of normokalemia and abnormal TTKG, further diagnosis may be needed, e.g., checking id the patient's diet is usual and not very rich or very low in potassium.
If you like our TTKG calculator, check our other urology tools:
- FEUrea calculator for fractional excretion of urea;
- FENa calculator for fractional excretion of sodium;
- Creatinine clearance calculator; and
- GFR calculator.